Glue ear (also known as secretory otitis media, otitis media with effusion, or serious otitis media) is a very common condition among children. This medical condition predominately occurs in children although it can develop at any age and can affect one or both ears.
How does the ear work?
The ear is divided into 3 parts – the outer, middle, and inner ear. Sound waves come into the outer (external) ear and hit the eardrum causing the eardrum to vibrate. Behind the eardrum, in the middle ear, are three tiny bones (ossicles) – the malleus, incus, and stapes. The vibrations pass from the eardrum to these middle ear bones. The bones then transmit the vibrations to the cochlea in the inner ear. The cochlea converts the vibrations to sound signals which are sent down the ear nerve to the brain which we ‘hear’.
The middle ear behind the eardrum is normally filled with air and is connected to the back of the nose by a thin channel, the Eustachian tube. This tube is normally closed. However, from time to time (usually when we swallow, chew or yawn), it opens to let air into the middle ear, and to drain any fluid out.
What is glue ear?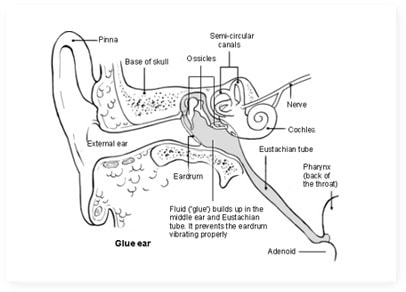
Glue ear occurs when the middle ear fills with a sticky, glue-like fluid instead of air. This fluid dampens the vibrations made by sound waves as they travel through the eardrum and ossicles. The cochlea in turn receives dampened vibrations, and so the ‘volume’ of hearing is essentially ‘turned down’. This is why glue ear children display symptoms such as dulled or apparent ‘selective hearing’.
Psychological effects
Some children can also experience psychological, developmental and behavioural effects as a result of dulled hearing caused by glue ear. If glue ear goes un-noticed it may mean children do not learn as well as they cannot hear their teacher. They may also become frustrated, feel left out and become quiet and withdrawn as they cannot follow what is going on around them as easily.
Although some studies have also shown glue ear may also potentially cause problems with speech and language development, this is unlikely to occur in most children with glue ear. However, if you have any concern about your child’s development, you should contact your GP.
Symptoms
The main symptom associated with glue ear is dulled hearing, which ranges from a slight muffle to moderately bad deafness in both ears to deafness in extreme cases. Below is a list of possible symptoms evident in glue ear children:
- Dulled hearing
- Problems with speech, language or social interaction
- Clumsiness or balance problems
- Appearing to have ‘selective hearing’ – for example, disobeying verbal instructions
- Turning up the volume on the television, or radio, or often saying ‘what’ or ‘uh’? a lot
- In the case of babies, being less responsive to sounds
Causes
A major cause of glue ear is thought to be due to the Eustachian tubes (which link the pharynx to the middle ear) not working correctly. If the Eustachian tube is narrow, blocked, or does not open properly, the balance of fluid and air in the middle ear may be altered. Once air gradually makes its way through the middle of the ear and passes into the nearby cells a vacuum will develop if the air is not replaced in the Eustachian tube. Additionally, fluid may also seep into the middle ear from nearby cells.
Often glue ear children develop the condition after an ear infection or contracting common illnesses such as colds, which encourages build-up of mucus. The mucus builds up in the middle ear and can struggle to drain down the Eustachian tube. However, many cases of glue ear are not the result of an ear infection.
Diagnosis
If you suspect your child has glue ear, you need to visit your GP. Your GP will ask about your child’s symptoms and medical history and then carry out a short ENT examination of your child focusing on the ear drums to evaluate whether an ear infection is present.
Typically, after this initial examination, your GP will send you away and ask you to return in one to three months to see if there’s been any improvement. This is called ‘watchful waiting’. If there hasn’t been any improvement over this period, your child is more likely to be referred to an Ear, Nose and Throat (ENT) specialist.
The Audiologist will perform a tympanometry test, which is the best available way to confirm glue ear. This test bounces sound waves off the ear drum and measures its flexibility. If the condition is judged severe enough your child will go on a waiting list for one of the main forms of glue ear treatment: a grommet operation. This takes place under full anaesthetic.
Information For Parents
- Watch our animated video with essential information for parents about glue ear. In this video you will learn everything you need to know about the condition and how it can be treated with Otovent®:
Otovent® is the only clinically effective, non-surgical, drug-free treatment for glue ear. The results from the latest clinical trial conducted by the University of Southampton show that children using Otovent® experienced fewer days with any glue ear related symptoms compared to those that didn’t at both one and three months.


